UPDATE: March 9, 2010 – Baclofen, the muscle relaxant and GABA agonist is being touted once more as a treatment for alcoholism. Read my thoughts on sibling science site SciScoop.com.
 As with much of medical science, the appearance of a fascinating research paper and an accompanying press release do not usually mean that a new pharmaceutical intervention, a medicine, is ready to be prescribed to patients on the very day that the paper appears. The drug discovery, research, and testing processes are much more long-winded than that.
As with much of medical science, the appearance of a fascinating research paper and an accompanying press release do not usually mean that a new pharmaceutical intervention, a medicine, is ready to be prescribed to patients on the very day that the paper appears. The drug discovery, research, and testing processes are much more long-winded than that.
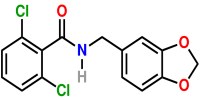
One example was a recent paper on Alda-1, the simplified name for N-(1,3-benzodioxol-5-ylmethyl)-2,6-dichlorobenzamide, a small organic molecule that activates the enzyme ALDH2 (aldehyde dehydrogenase 2). ALDH2 is involved in metabolising the aldehyde byproducts of other substances in the body particularly alcohol.
In September 2008, Alda-1 was touted by the media as a “new drug hope for controlling heart damage”. By activating ALDH2 it was suggested that those people who have an inactive form of that enzyme (some 40% of East Asians and people of East Asian descent) could be treated with the compound to preclude the cardiotoxicity of aldehydes formed when they drink alcohol.
More recently, the same researchers involved in the 2008 study, Thomas Hurley of the University School of Medicine in Indianapolis and Daria Mochly-Rosen, of Stanford University School of Medicine, and colleagues, have published a crystallographic study showing more details of how Alda-1 works to activate ALDH2. You can read my write-up on this work today in the latest issue of the X-ray ezine on SpectroscopyNOW.com.
However, press releases are notoriously hopeful about the actual use to which a piece of biomedical research might be put so I asked Hurley for some additional insight into the likely fortunes of Alda-1.
“Alda-1 is not ready for human trials, nor is it ever likely to be,” he told me. “Its potency is relatively low for an effective in vivo agent, especially when one accounts for its solubility.”
The compound is, as those in pharma research will have realised from the off, simply a lead compound. A compound that researchers will use as the starting point for novel and potentially more efficacious and more soluble compounds, analogues, that would be designed for testing and clinical trials.
“We have much work to do on this before clinical trials can even start to evaluate whether this is an effective strategy in vivo,” conceded Hurley, “I doubt there will anything ready for clinical application for 7-10 years, unless we get really lucky here in the next year with our analogue design and testing,” he adds.
One thing that the original media attention did get right is that Alda-1 might eventually lead to a primary clinical application in the area of cardioprotective effects. This would be rather than it being developed as a drug to allow East Asian drinkers with the ALDH2 mutation to imbibe more alcohol than their flush response, nausea, and palpitations would normally allow them.
“Its use as an activator for alcohol metabolism will, hopefully, be regulated,” Hurley told me, “There are broad ethical issues associated with an application toward reducing alcohol intolerance in the East Asian population or individuals of East Asian descent.”
He points out that pescribing a drug descended from Alda-1 to activate mutant ALDH2 would be like curing a lifestyle issue (alcohol intolerance) and replacing it with an increased risk for a devastating disease – alcoholism. “Currently, there is relatively low risk of alcohol abuse or alcoholism in those individuals who are intolerant to ethanol consumption, so ‘curing’ the intolerance is very likely to lead to an increase in the prevalence of these devastating diseases in these low risk populations,” Hurley added.
Once a drug is developed for the cardioprotective benefits emerges on to the market, however, you can bet your last Yen that a blackmarket will quickly emerge where there are large populations of East Asians, for a pill that would allow otherwise lightweight drinkers to put themselves under the table without the flushing, nausea and palpitations. Of course, it won’t ever preclude the need to consider the health risks of excessive drinking and to seek alcohol treatment if one’s drinking becomes a serious problem.
![]() Perez-Miller, S., Younus, H., Vanam, R., Chen, C., Mochly-Rosen, D., & Hurley, T. (2010). Alda-1 is an agonist and chemical chaperone for the common human aldehyde dehydrogenase 2 variant Nature Structural & Molecular Biology DOI: 10.1038/nsmb.1737
Perez-Miller, S., Younus, H., Vanam, R., Chen, C., Mochly-Rosen, D., & Hurley, T. (2010). Alda-1 is an agonist and chemical chaperone for the common human aldehyde dehydrogenase 2 variant Nature Structural & Molecular Biology DOI: 10.1038/nsmb.1737